


LONDON: It is more than 60 days since China first alerted the World Health Organization (WHO) to the emergence of a mysterious new virus in the city of Wuhan.
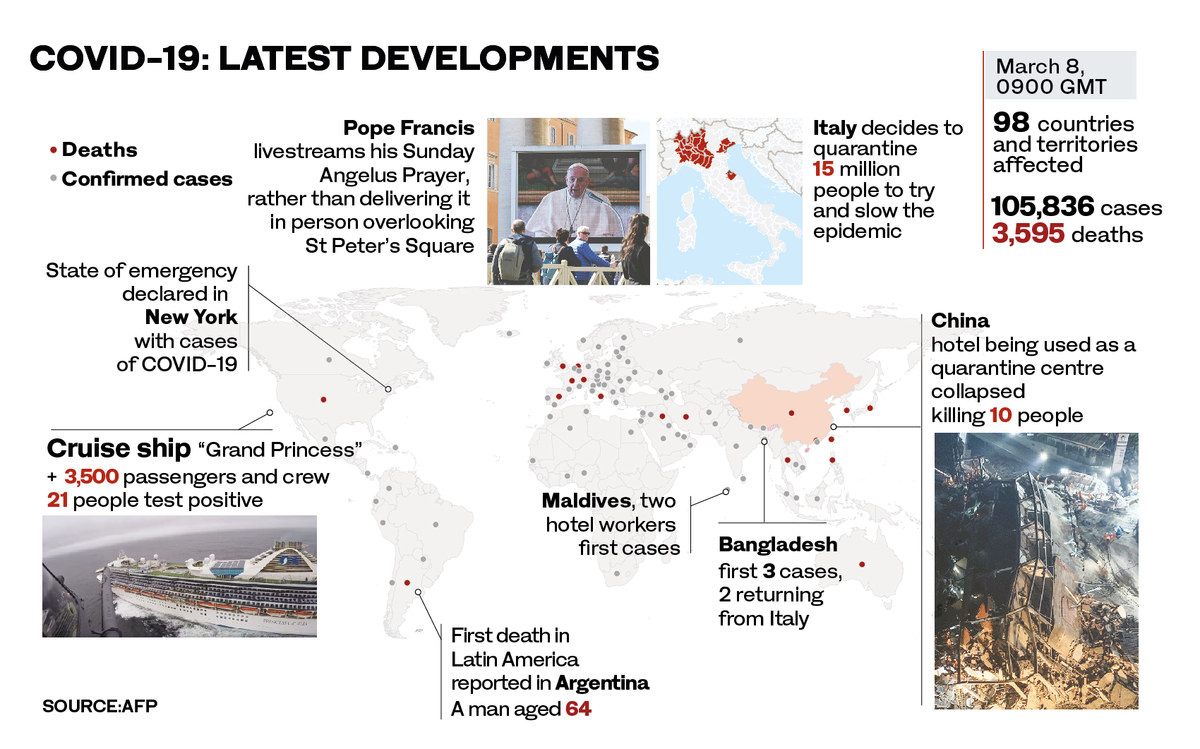
Since then, the virus has been identified and named — SARS-CoV-2. It has infected more than 100,000 people around the world, caused more than 3,000 deaths, shaken stock markets and prompted predictions of job losses, shortages of food and medicines and even a global economic meltdown.
Certainly, fear of the coronavirus disease 2019 (COVID-19) is affecting events and organizations around the globe, from the cancelation of football matches and conferences to the closure of Asian theme parks and museums in Italy and France.
Saudi Arabia has temporarily stopped entry into the Kingdom by land from three GCC neighbors, with the Ministry of Sports suspending public attendance at all sports events.
Inevitably, a shadow hangs over other major international events, from the summer’s Tokyo Olympic Games to Expo 2020 in Dubai, due to open in October.
FASTFACTS
People in coronavirus-affected countries should avoid large gatherings, handshakes or hugs, maintain “social distancing” from others, cover their nose and mouth while coughing or sneezing, and wash their hands regularly.
Many people who contract the coronavirus will have no symptoms or only a mild version of the disease.
Most deaths so far have been among the elderly or others with long-term health conditions.
The risk of dying after contracting the coronavirus is just 0.9% for someone with no other health conditions, 5.6% for cancer patients.
The risk is 6% for people with high blood pressure, and 7.3% and 10.75% for individuals with chronic respiratory disease and cardiovascular disease respectively.
Despite the WHO’s reluctance to classify the outbreak as a pandemic — a disease that has spread globally — most epidemiologists believe that the window of opportunity for limiting the spread of the disease by banning flights to and from infected countries or shutting borders has long closed.
Is the coronavirus worse than SARS or Middle East Respiratory Syndrome (MERS)? Yes. In two months, it has killed almost twice as many people as those two viral diseases combined, and many epidemiologists believe that the coronavirus will continue spreading widely.
Clearly, the emphasis must now shift to controlling it within individual countries via swift identification and isolation of cases, and the equally rapid tracing, testing and, if necessary, isolating of anyone with whom infected people have come into contact.
For even the best health care systems, this is a challenging task, the success of which will be dependent on a series of still unknown variables.
As virologists around the world race to produce a vaccine — and there is no guarantee that one will be found — so epidemiologists are developing best-guess answers.
One of the teams most experienced in this field is at the Center for the Mathematical Modelling of Infectious Diseases at the London School of Hygiene & Tropical Medicine, where a coronavirus working group is running computer models to look at outcomes based on a range of possibilities.
The team’s initial conclusion, that “in most scenarios, highly effective contact tracing and case isolation is enough to control a new outbreak of COVID-19 within 3 months,” sounds reassuring. But, as their paper published last week in the journal Lancet Global Health points out, success will depend on exactly which scenario emerges.
The findings suggest two crucial steps that every country currently with one or more cases should be taking. Although logistically and economically challenging, the best hope of control lies in mass population testing to identify and isolate infected people before symptoms emerge.
Opinion
This section contains relevant reference points, placed in (Opinion field)
Resources should also be invested now in creating effective contact-tracing teams. Until more is known about the incubation period of the virus, according to evidence so far patients should be isolated for at least two weeks, and possibly three.
The coronavirus is, of course, not the first epidemic to trigger global panic, but we should take heart from our experience of those that have come before.
Although no longer in the headlines, neither SARS nor MERS, which are genetically related but in many ways different to the coronavirus, have gone away, but thanks to timely and effective intervention failed to live up to their apocalyptic billing.
SARS, which was first reported in Asia in February 2003, spread to two dozen countries, infecting 8,098 people worldwide and killing 774, before the outbreak was contained in July the same year.
The virus succumbed to strict isolation, quarantine and tracing of contacts and there have been no known cases anywhere in the world since 2004.
MERS, first identified in Saudi Arabia in 2012, continues to kill, but on a much-reduced scale. Between Dec. 1, 2019, and Jan. 31, 2020, Saudi Arabia reported 19 cases of MERS infection, with eight deaths, bringing the total number of cases globally since 2012 to 2,521, with 919 deaths.
But although the new coronavirus is related to the others, each operates in subtly different and potentially confounding ways, which makes lessons learnt from one difficult to apply to another.
For example, the Spanish flu was an unusually deadly strain of avian influenza, a viral infectious disease that killed possibly 50 million people worldwide over about a year in 1918 and 1919.
With SARS, symptoms came on rapidly, which meant cases could be identified quickly, leading to swifter and more effective isolation and treatment.
When swine flu, the disease caused by the then-novel H1N1 virus, emerged in the US in April 2009, the world again seemed to be facing a pandemic disaster. In the event, swine flu infected one-tenth of the global population and killed as many as 575,400 people worldwide. But by August the following year the WHO declared it had run its course.
Today swine flu is just one of the seasonal influenzas that flare up annually around the world, which is not to say it is of no consequence. Every year, despite vaccines, various mutating strains of flu infect an estimated four million people, causing almost half a million deaths.
We have, in other words, learnt to live with flu, a grim reality that should at least help us to put into perspective the threat posed by the coronavirus.
Most of the fatalities so far have been in China, where the disease originated, and experience with other coronaviruses tells us that if effective control measures are put in place in other countries, we can limit the damage.

A couple wearing facemasks smear their faces with colored powder to celebrate Holi, the Hindu spring festival of colours, in Hyderabad. (AFP)
There are, however, still many uncertainties about the true scale of the spread of the virus.
For a start, because many people seem to contract only a mild case of the coronavirus, it is certain that the incidence of the disease around the world is being significantly under-reported.
Many carriers will have no symptoms and even those with only a “lite” version of the key symptoms — a slightly elevated temperature, tiredness and dry cough — will not visit a doctor, will recover without medical help and will not be counted in the statistics.
The upside of this is that the overall death rate from the disease — currently provisionally estimated at 2 or 3 percent — is undoubtedly exaggerated. The downside is that these silent carriers can still spread the disease, undetected.
For now, the immediate future course of the coronavirus cannot be predicted with any accuracy and we certainly cannot assume it will go the same way as swine flu, MERS or SARS.
On March 2, when WHO raised its assessment of the threat of the coronavirus to the highest level, Michael Ryan, director of health emergencies, said that this was a reality check for every government in the world.
“Wake up. Get ready,” he said. “This virus may be on its way, and you need to be ready.”
This time, luck might not be on our side.



















